Anatomical Short Leg Length
Altered Biomechanics and Altered Gait
Future Joint Degeneration and Future Back Pain
Following the discovery of x-rays in 1895 (by German physicist Wilhelm Conrad Roentgen), x-rays of the spine began to appear in healthcare research and literature. In 1916, Harvard Orthopedic Surgeon Robert W. Lovett, MD, published the third edition of his book Lateral Curvature of the Spine and Round Shoulders (1). This text has many examples of spinal radiographs, showing a biomechanical relationship between leg length, pelvic leveling, spinal scoliosis, and back pain.
In 1946, in the largest study at that time, Lieutenant Colonel Weaver A. Rush and Captain Howard A. Steiner of the X-ray Department of the Regional Station Hospital of Fort Leonard Wood, Missouri, meticulously exposed upright lumbosacral x-rays on 1,000 soldiers. The results of this study were published in the American Journal of Roentgenology and Radium Therapy, titled (2):
A Study of Lower Extremity Length Inequality
The authors made these findings:
- Only 23% of the soldiers had legs of equal length.
- 77% of the soldiers had unequal length of their legs, and of that 77%, 36% had a deficiency greater than 5 mm.
These authors found that the short leg was associated with a downward tilt of the pelvis and a compensatory scoliosis. They noted:
“Because this scoliosis, in all instances, compensates for the tilt of the pelvis, it is referred to by us as compensatory scoliosis.”
“The existence of this compensatory scoliosis in the presence of a tilted pelvis due to shortening of one or the other lower extremity is believed by us to have clinical significance and, furthermore, it is our opinion that the existence of any such condition cannot be determined with any degree of accuracy on gross physical examination.”
“Furthermore, it becomes immediately apparent that the making of roentgenograms of the lumbosacral spine in the recumbent position, as is frequently done, completely prevents the discovery of such pathology as this.”
“It was a general consistent observation that the degree of scoliosis was proportionate to the degree of pelvic tilt. An individual who has a shortened leg will have to compensate completely if he intends to hold the upper portion of his body erect or in the midsagittal plane.”
“A consistent observation which has been made is that in those cases with a shortened leg there is a corresponding tilt of the pelvis and a compensatory scoliosis of the lumbar spine.”
Leg length differences exceeding 5 mm were associated with greatest low back pain or disability, and therefore 5 mm is labeled as being a “marked difference.” The authors stated:
“For this reason, it is our opinion that the existence of such a condition [a short leg exceeding 5 mm] is significant from the standpoint of symptomatology and disability.”
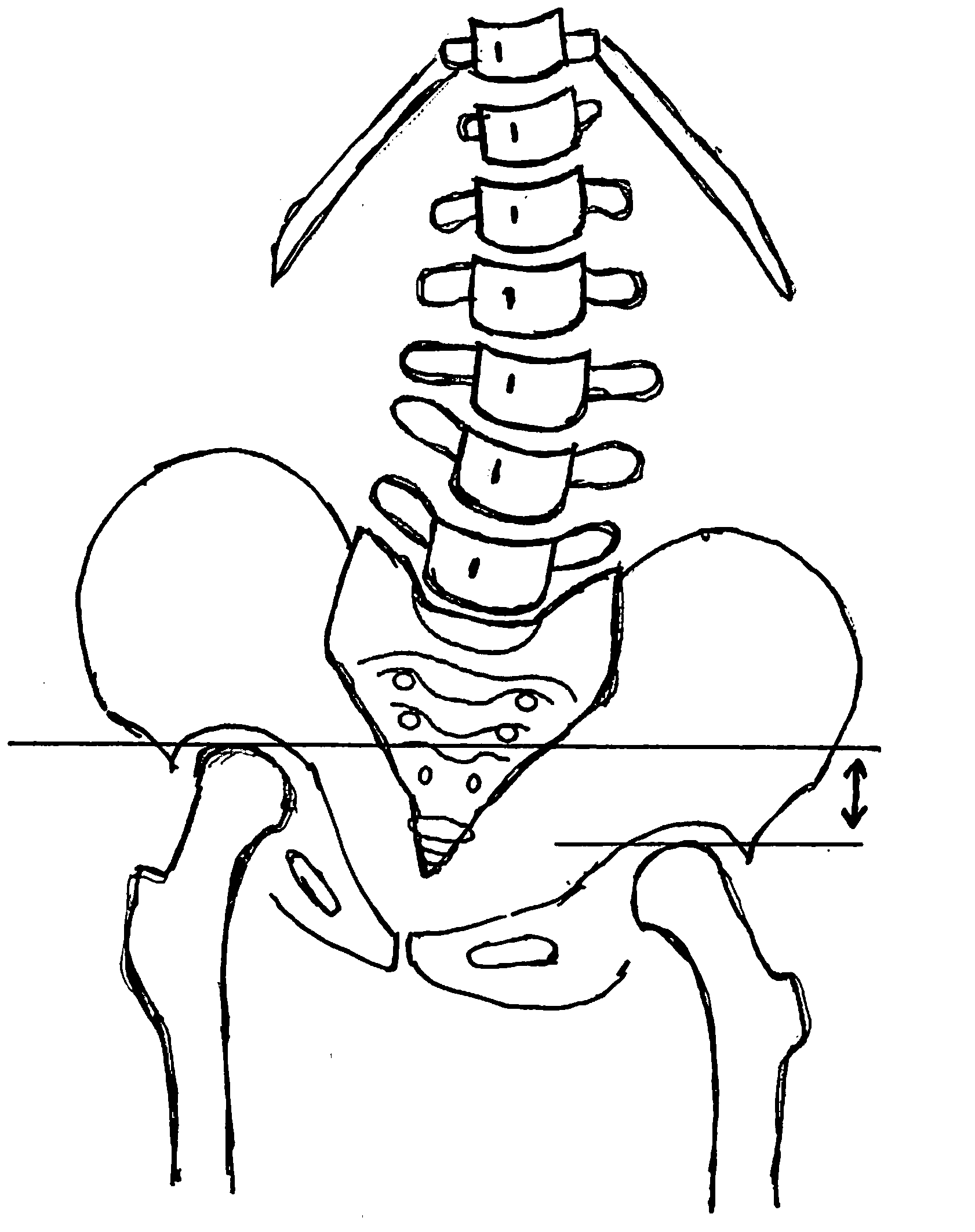
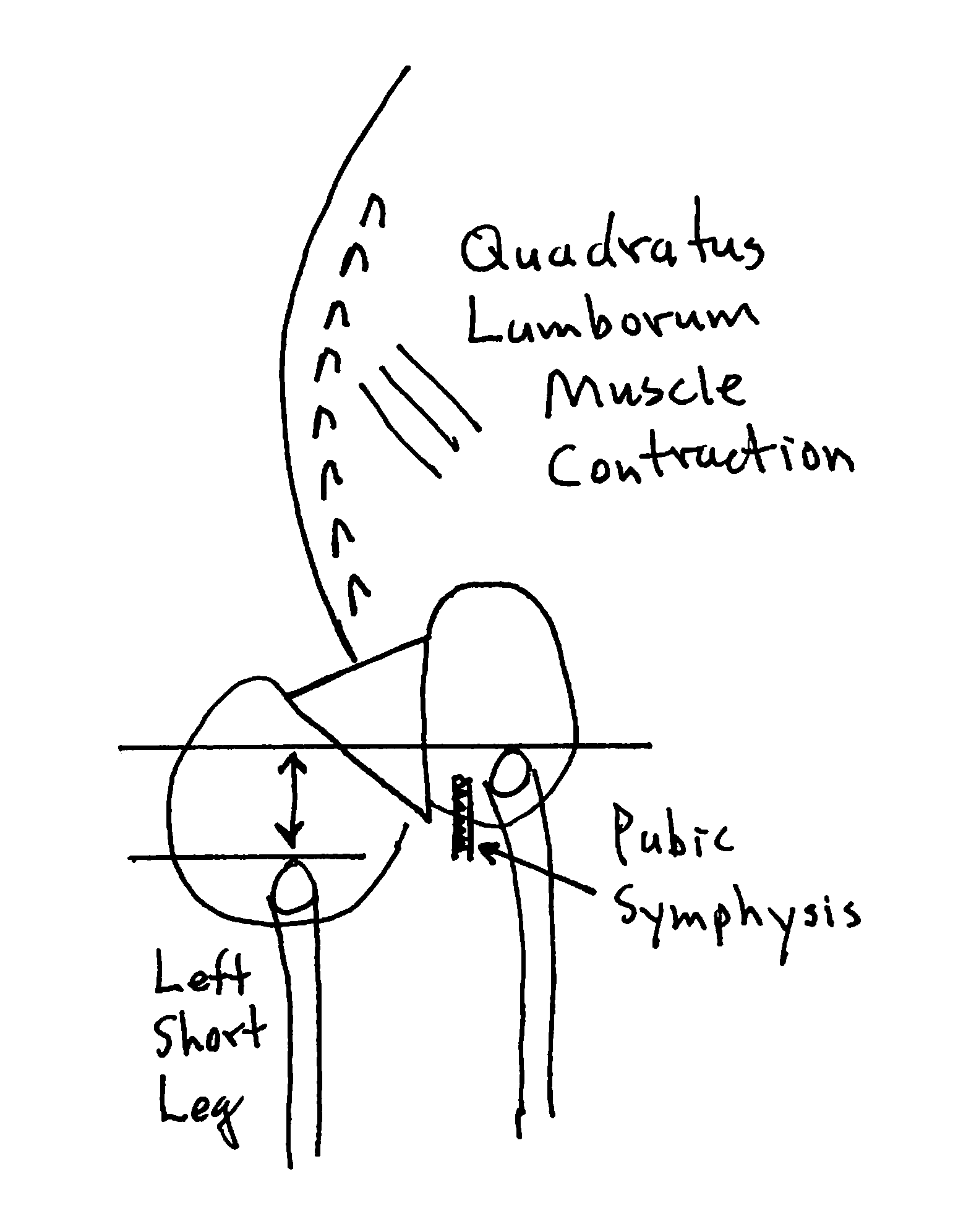 Posterior to Anterior View from Behind
Posterior to Anterior View from Behind
- The sacrum is lower on the side of the short left leg.
- The spinal column initially tilts towards the short leg, then compensates back to the midline as a consequence of contraction of the quadratus lumborum.
- The lumbar spinous processes (posterior) rotate towards the long leg. The pubic symphysis (anterior) also rotates towards the long leg. The consequent counter-rotational forces abnormally stress the L5 intervertebral disc.
••••
In 1970, a study was published in the American Journal of Obstetrics and Gynecology, titled (3):
The Short Leg Syndrome in Obstetrics and Gynecology
The authors note that an anatomical short leg can cause chronic low back and flank pain, and that “many women had been subject to hysterectomy, uterine suspension, and presacral neurectomy with poor results.” The pain is because of imbalance causing traction on the abdominal, paravertebral, and gluteal muscles. The pain is “increased when standing, during exercise, and after physical exertion, and is generally relieved by rest.” The authors found that treatment with the application of a lift to the heel of the short leg resulted in:
“Relief was usually prompt and in most instances no more than 2 weeks [was] necessary for complete adjustment. The results of applying a heel lift on the short leg were excellent in 90% of the patients.”
••••
In 1981, an article was published in the journal Spine and titled (4):
Low-back Pain Associated with Leg Length Inequality
After establishing a precise, accurate radiological measurement for the anatomical short leg in patients with chronic low back pain, the authors assessed the clinical outcomes for these patients that used the shoe-lift intervention. The authors found:
- Limb length inequality was an important factor in the production of low back pain.
- Using shoe-left therapy on the short limb reduced the number of attacks of low back pain and the number of working days lost to low back pain.
••••
In 1983, a study was published in the journal Spine, titled (5):
Clinical Symptoms and Biomechanics of Lumbar Spine
and Hip Joint in Leg Length Inequality
The author details the relationship between an anatomical short leg, back pain, and spinal biomechanics by exposing upright weight-bearing radiographs on 1,157 subjects. The author found that leg length inequality became clinically relevant at 5 mm, noting:
In 79% of those with chronic or recurrent sciatic pain, the symptoms occurred on the side of the longer lower extremity.
In 89% of those with unilateral hip pain, the symptoms occurred on the side of the longer leg.
“When correcting the leg length inequality simply with an adequate shoe lift, a permanent and mostly complete alleviation of symptoms was achieved in the majority of the cases.”
••••
In 1985, a study was published in the Journal of Rheumatology, titled (6):
Persistent Low Back Pain and Leg Length Disparity
The author notes that short leg causing low back pain is a chronic problem that comes on within 20 or 30 minutes of being upright and is relieved quickly with sitting. The best treatment is the insertion of an appropriate heel lift. The author states:
“The suggestion that leg length disparity can produce low back pain has been known since before the turn of the century and although lip service has been paid to it by physicians it is not a matter taught in medical schools nor addressed seriously by most physicians.”
“A radiological method in which the femoral head heights are measured on an AP radiograph of the pelvis taken in the erect position has shown to be reproducible.”
••••
In 1985, a study was published in the journal The Practitioner, titled (7):
Leg Length Inequality and Low Back Pain
In this article the author notes:
“A permanent shoe raise to the shorter leg improved the symptoms in the majority of the patients.”
“This supports the view that leg length is a readily identifiable and easily correctable cause of chronic back pain.”
••••
In 1987, a study was published in the journal Radiological Medicine, in Italian. The English translation of the title is (8):
Radiological Findings in Idiopathic Scoliosis
The English abstract of this articles states:
“Following radiological investigations of the spine and pelvis, carried out in the standing position on 5000 young and adult subjects, the author reports a series of radiological features from which it appears clear that the inequality in length of lower extremities is the primary cause of that complex mechanism which is responsible of apparently idiopathic scoliosis.”
••••
In 1987, an article was published in the journal Clinical Biomechanics, titled (9):
The Statics of Postural Pelvic Tilt Scoliosis:
A Radiographic Study on 288 Consecutive Chronic LBP Patients
The author exposed standing radiographs of the pelvis and lumbar spine in 288 consecutive patients with chronic low back pain and in 366 asymptomatic controls. He noted:
“[In 91.4% of cases], the lumbar curve was convex toward the short leg side, correlating significantly with the degree of lateral inclination of the sacrum and with the amount of leg length inequality. The curvature was generally coupled with an axial rotation of the vertebrae moving the spinous processes toward the concavity, as well as with an opposite rotation of the pelvis, which were calculated to result in a significant torsional stress on the L5-S1 segment.”
••••
In 2000, a chapter was published in the book SPINE: State of the Art Reviews. The chapter was titled (10):
Lower Limb Length Inequality and Scoliosis
in Etiology of Adolescent Idiopathic Scoliosis
The author notes:
“During growth, LLLI, even of the order of just a few mm, can cause a tilt of the pelvis and consequently lateral deviation of the spine and head. The postural response, aimed at re-establishing equilibrium, is a compensatory counter-deviation of the spine.”
“In the treatment of scoliosis, the compensation of LLLI using a lift under the heel of the shorter limb is always useful and effective [in compensatory curves].”
“The overload at the lumbosacral level may produce muscular stress, premature degenerative diseases of the disc or somatic structures and the interapophyseal joints L4-L5 and/or L5-S1, as well as dysfunction of the sacroiliac joint, which might give rise to low back and pelvic pain of mechanical origin.”
••••
In 2005, a study was published in the journal Archives of Physical Medicine and Rehabilitation, titled (11):
Conservative Correction of Leg-Length Discrepancies
of 10 mm or Less for the Relief of Chronic Low Back Pain
The authors note that mild leg-length discrepancy of 10 mm or less is common, found in 96% of the adult population. Leg-length discrepancy as small as 2 mm can be clinically significant.
Leg-length discrepancy causes asymmetry in the lower-extremity joints and in the spine and pelvis, leading to stress and strain with a derangement of normal biomechanical function, postural scoliosis, stress on facet joints and discs, resulting in degenerative changes.
Shoe inserts significantly reduced both pain intensity and disability in patients with chronic low back pain and a short leg of 10 mm or less. In this study, 96% of those treated with a shoe insert for chronic low back pain achieved complete pain resolution or significant pain resolution within 12 weeks.
Shoe inserts are recommended to be included in the treatment of patients with chronic low back pain when they have mild leg-length discrepancy.
••••
In 2007, a study was published in the Journal of Orthopaedic & Sports Physical Therapy, titled (12):
Changes in Pain and Disability Secondary to Shoe Lift Intervention
in Subjects with Limb Length Inequality and Chronic Low Back Pain
The authors note that limb length inequality (LLI) may be a cause of low back pain (LBP). Patients with LLI often have increased pain from standing for 20 to 30 minutes, followed by immediate relief upon sitting.
Multiple studies report higher prevalence of LLI in individuals with LBP compared to control subjects. Evidence to support the association between LLI and LBP is provided by studies showing significant improvement in patient’s low back symptoms following insertion of a shoe lift. Typically, the reduction in chronic LBP pain and improvement in function was noted approximately 1 week following establishment of final lift intervention height. The authors conclude:
“Shoe lifts may reduce LBP and improve function for individuals who have chronic LBP and an LLI.”
••••
In 2016, a study was published in the Journal of Craniovertebral Junction Spine, titled (13):
Inequality in Leg Length is Important for the Understanding
of the Pathophysiology of Lumbar Disc Herniation
These authors evaluated 39 subjects with leg length discrepancy and low back pain and 43 controls to quantify the occurrence of disc herniation between the two groups. They concluded that leg length inequality causes spinal joint load asymmetry, accelerating disc degeneration and disc herniation. They also suggest the poor low back disc surgical outcomes may be linked to the abnormal spinal loads caused by leg length inequality. They note:
“Inequality in leg length may lead to abnormal transmission of load across the endplates [causing] degeneration of the lumbar spine and the disc space.”
“Human coronal balance may be one of the causes of operative failure after disc surgery. Assessment of pathologic coronal imbalance requires a clear understanding of normal coronal alignment.”
“Patients with chronic LBP have a minor balance defect. Inequality in leg length is important for the understanding of the pathophysiology of lumbar disc degeneration and herniation.”
“Our observations suggest that LBP may have etiologies related to abnormal load transmission due to coronal imbalance. It seems that a successful treatment may sometimes exist beyond good surgery. In these situations, abnormal coronal balance may be an important factor.”
••••
In 2017, a study was published in the journal Archives of Physical Medicine and Rehabilitation, titled (14):
Shoe Orthotics for the Treatment of Chronic Low Back Pain:
A Randomized Controlled Trial
The objective of this study was to investigate the efficacy of shoe orthotics with and without chiropractic treatment for chronic low back pain as compared to no treatment. It is a randomized controlled trial that involved 225 adults with symptomatic low back pain of 3 months or longer. These authors note:
“This large-scale clinical trial demonstrated that LBP and disability were significantly improved after six weeks of orthotics care compared to a wait-list control, and that the addition of chiropractic care with the orthotics demonstrated a significant improvement in the disability scores compared to orthotics alone.”
“Six weeks of prescription shoe orthotics significantly improved back pain and dysfunction compared to no treatment. The addition of chiropractic care led to higher improvements in function.”
“Foot dysfunction should not be overlooked as a potential contributing factor in treating individuals with LBP and dysfunction.”
••••
In 2018, a study was published in the Journal of Bone and Joint Surgery Reviews, titled (15):
Leg-Length Discrepancy, Functional Scoliosis, and Low Back Pain
The authors note that leg-length discrepancy results in a functional scoliosis when the lumbar spine compensates for pelvic obliquity to maintain shoulder balance.
The authors define a functional scoliosis as one that corrects when an appropriate heel lift is placed under the shorter leg:
“When evaluating a patient with leg length discrepancy and scoliosis radiographically, a true functional scoliosis will correct completely or partially when the pelvis is leveled with blocks placed under the short leg.”
They note that in addition to the functional scoliosis, patients with leg length discrepancy also often suffer from lower back pain. They note that the standard evaluation of these patients is radiographic. These radiographs are taken both initially when the leg length discrepancy is posturally suspected, and again after the use of heel lifts to assess correction. They state:
“Patients with leg length discrepancy, low back pain, and functional scoliosis should undergo radiographic evaluation with the pelvis leveled using blocks placed under the shorter limb.”
In children, asymmetries of weight-bearing adversely affect the growth plates of the weight-bearing bones, especially the legs and the spinal vertebra. These growth asymmetries tend to be asymptomatic. Yet, they may be the cause of adult symptomatology and adult degenerative changes. These authors state:
“While children typically do not complain of low back pain in the setting of leg length discrepancy, the available evidence suggests that long-standing leg length discrepancy may cause permanent changes in lumbar spine biomechanics, predisposing these patients to future low back pain and degenerative scoliosis.”
Long standing leg length discrepancy and asymmetries of weight bearing are associated with acceleration of articular degenerative changes as well as histological and functional changes in the counter-balancing musculature. These authors note the following:
“Pelvic tilt and compensatory, or functional, scoliosis in the short term resulted in asymmetrical loading of the intervertebral discs and facet joints in the lumbar spine.”
“Patients with leg length discrepancy had a significantly increased prevalence of degenerative joint disease at the L5/S1 spinal motion segment and at the L4/L5 segment compared with cohorts without leg length discrepancy.”
“Long-standing leg length discrepancy may result in degenerative changes of the lumbar spine, altered gait mechanics, and low back pain.”
“Long-standing abnormal spinal biomechanics were thought to result in degenerative disc disease and permanent changes in the lumbar spine.”
“Superimposed functional scoliosis is likely to result in accelerated disc degeneration.”
“When L5/S1 segment degeneration was evaluated as a function of age, men [over] 50 years old with leg length discrepancy had a significantly increased prevalence of degenerative changes compared with an age-matched cohort without leg length discrepancy.”
“There is evidence to support leg length discrepancy as a cause of persistent biomechanical changes in the lumbar spine, and those biomechanical abnormalities may result in permanent degenerative changes to the vertebral bodies.”
“Long-duration functional scoliosis may result in permanent biomechanical changes in the lumbar spine.”
“There is a correlation, if not a cause-and-effect relationship, between pelvic obliquity and degenerative scoliosis resulting in lumbar spine surgery.”
These authors note that the best initial approach for the management of patients with leg length discrepancy, symptomatology, and/or disability is the insertion of an appropriate shoe lift.
••••
In 2025, a study was published in the journal Gait & Posture, titled (16):
Impact of Mild Leg Length Discrepancy
on Pelvic Alignment and Gait Compensation in Children
This study aimed to identify gait deviations in children and adolescents with mild leg length discrepancy (LLD) and examine the relationship between LLD severity and lower limb compensatory strategies. They assessed 51 subjects with a mean age of 12 years, with a full-limb anterior-posterior standing radiograph. The authors note:
“Leg length discrepancy (LLD) is common in children and often leads to pelvic lateral tilt as a primary gait deviation.”
“Pelvic lateral tilt is the most frequently seen gait deviation during walking due to LLD and is a common cause for a functional scoliosis with concavity to the side of the longer limb.”
“While children typically do not complain of low back pain, long-standing LLD may cause permanent changes in lumbar spine biomechanics, predisposing these patients to future low back pain and degenerative scoliosis.”
“Even mild discrepancies may contribute to overuse injuries affecting the spine and longer limb.”
“Our results support the notion that interventions utilizing shoe soles can effectively reduce pelvic tilt and improve ankle dorsiflexion, highlighting these strategies as essential for mild LLD.”
“The observed strategies are directly related to the severity of LLD, indicating that even mild LLD is not naturally compensated for and may lead to overuse problems in the spine and the longer limb.”
“These pelvic adaptations subject the lumbosacral junction to increased pathological loading and asymmetrical movements, potentially contributing to the development of lower back pain depending on daily activities and sports involvement.”
“When patients report low back pain, LLD should be considered as a potential contributing factor.”
“Correcting mild LLD with an appropriate shoe lift has been shown to provide lasting and often complete symptom relief in most cases, further supporting the causative link between small LLD and lower back pain.”
SUMMARY
For individuals suffering from chronic low back pain, the combination of shoe lifts to compensate for leg length discrepancy, and chiropractic spinal adjusting (specific manipulations) to the spinal joints appears to be a biologically sound management approach. This is especially appropriate for those with chronic low back pain that is treatment resistant. This approach may prevent low back pain and disc disease/herniation, and improve surgical outcomes.
REFERENCES
- Lovett RW; Lateral Curvature of the Spine and Round Shoulders; Third edition; P. Blakiston’s Son & Co; Philadelphia; 1916.
- Rush WA, Steiner HA; A Study of Lower Extremity Length Inequality; American Journal of Roentgenology and Radium Therapy; November 1946; Vol. 51; No. 5; pp. 616-623.
- Sicuranza B, Richards J, Tisdall L; The Short Leg Syndrome in Obstetrics and Gynecology; American Journal of Obstetrics and Gynecology; May 15, 1970; Vol. 107; No. 2; pp. 217-219.
- Giles LG, Taylor JR; Low-back Pain Associated with Leg Length Inequality; Spine; Sep-Oct 1981; Vol. 6; No. 5; pp. 510-521.
- Friberg O; Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality; Spine; September 1983; Vol. 8; No. 6; pp. 643-651.
- Gofton JP; Persistent Low Back Pain and Leg Length Disparity; Journal of Rheumatology; August 1985; Vol. 12; No. 4; pp. 747-750.
- Helliwell M; Leg Length Inequality and Low Back Pain; The Practitioner; May 1985; Vol. 229; pp. 483-485.
- Manganiello A; Rilievi Radiologici Nelle Scoliosi Idiopatiche; Radiological Med (Torino); April 1987; Vol. 73; No. 4; pp. 271-276.
- Friberg O; The Statics of Postural Pelvic Tilt Scoliosis: A Radiographic Study on 288 Consecutive Chronic LBP Patients; Clinical Biomechanics; November 1987; Vol. 2; No. 4; pp. 211-219.
- Manganiello A; “Lower Limb Length Inequality And Scoliosis, in Etiology of Adolescent Idiopathic Scoliosis” SPINE: State of the Art Reviews; May 2000; Vol. 14; No. 2.
- Defrin R, Benyamin SB, Dov Aldubi R, Pick CG; Conservative Correction of Leg-Length Discrepancies of 10 mm or Less for the Relief of Chronic Low Back Pain; Archives of Physical Medicine and Rehabilitation; November 2005; Vol. 86; No. 11; pp 2075-2080.
- Golightly YM, Tate JJ, Burns CB, Gross MT; Changes in Pain and Disability Secondary to Shoe Lift Intervention in Subjects with Limb Length Inequality and Chronic Low Back Pain; Journal of Orthopaedic & Sports Physical Therapy; July 2007; Vol. 37; No. 7; 380-388.
- Balik SM, Kanat A, Erkut A, Ozdemir B, Batcik OE; Inequality in Leg Length is Important for the Understanding of the Pathophysiology of Lumbar Disc Herniation; Journal of Craniovertebral Junction Spine; April-June 2016; Vol. 7; No. 2; pp. 87-90.
- Cambron JA, Dexheimer JM, Duarte M, Freels S; Shoe Orthotics for the Treatment of Chronic Low Back Pain: A Randomized Controlled Trial; Archives of Physical Medicine and Rehabilitation; September 2017; Vol. 98; No. 9; pp. 1752-1762.
- Sheha ED; Steinhaus ME; Kim HJ; Cunningham ME; Fragomen AT; Rozbruch SR; Leg-Length Discrepancy, Functional Scoliosis, and Low Back Pain; Journal of Bone and Joint Surgery Reviews; August 8, 2018; Vol. 6; No. 8; pp. e6.
- Bohm H, Dussa CU; Impact of Mild Leg Length Discrepancy on Pelvic Alignment and Gait Compensation in Children; Gait & Posture; May 2025; Vol. 118; pp. 122–129
“Authored by Dan Murphy, D.C. Published by ChiroTrust® – This publication is not meant to offer treatment advice or protocols. Cited material is not necessarily the opinion of the author or publisher.”
